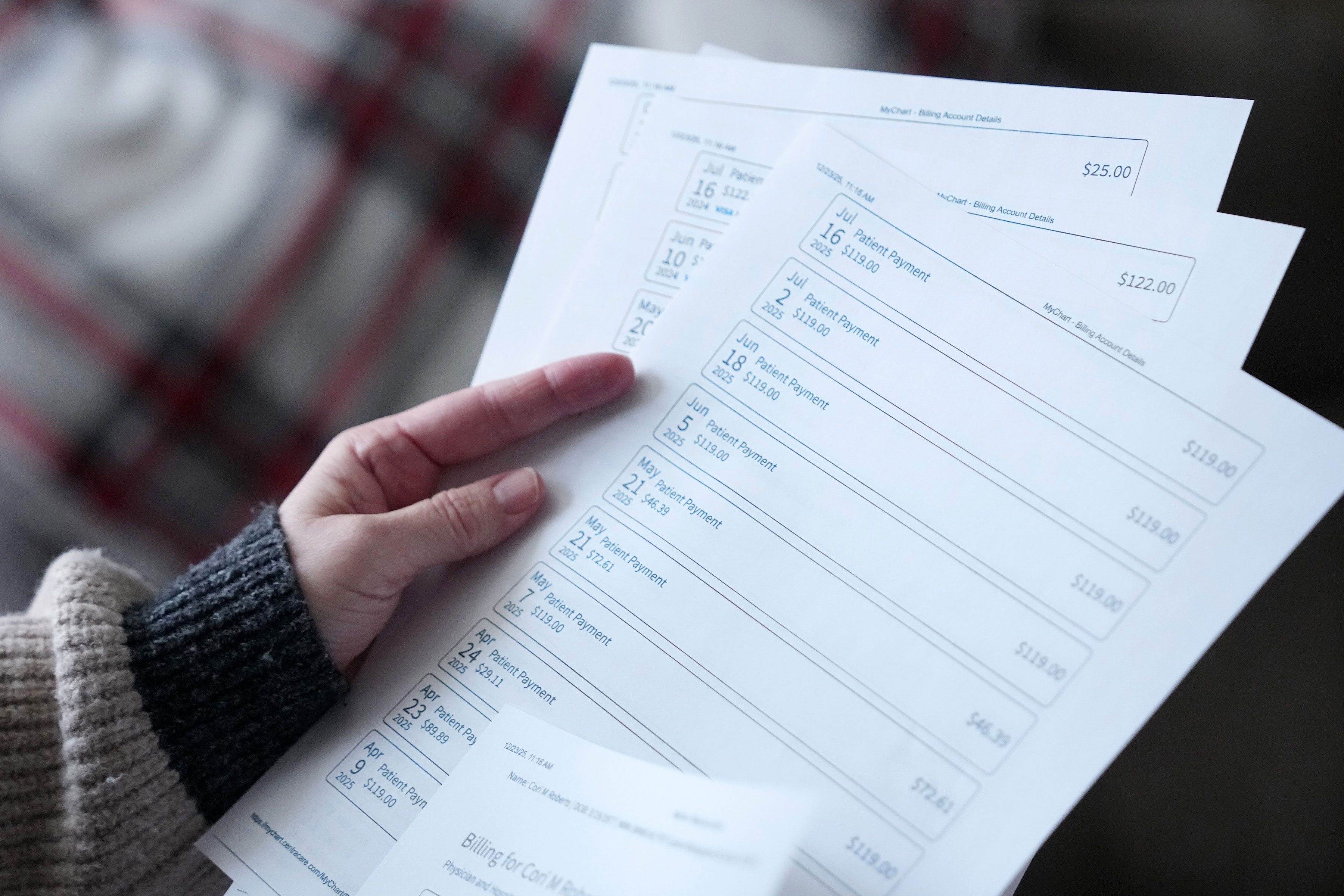
ST. CLOUD, Minn. — Cori Roberts was living in a rented basement four years ago when she was diagnosed with early-stage cervical cancer.
Recently divorced, the former stay-at-home mother had started working again in her mid-40s, taking a human resources job that paid $41,000 a year. Then, despite having insurance, she was hit with more than $8,000 in medical bills.
“I had my car and a basket of clothes,” Roberts recalled. “Medical bills were not something I could have afforded.”
Roberts sought financial assistance from CentraCare, the St. Cloud-based health system that treated her. It’s a nonprofit charity that receives millions of dollars in federal, state, and local tax breaks. In exchange, it’s obliged to offer charity care to patients who can’t afford their medical bills. But Roberts said CentraCare told her she made too much to qualify.
Roberts instead scrimped on groceries and Christmas gifts for her kids and paid off more than $6,000 over two years. Then CentraCare sued her last year because she hadn’t paid off all the debt.
“They’re supposed to be a nonprofit,” Roberts said. “It’s like, ‘Come on!’”
CentraCare earmarks a tiny fraction of its budget for helping patients with medical bills they can’t pay, but it’s not alone, a Minnesota Star Tribune-KFF Health News investigation found.
Minnesota’s hospitals and health systems are among the least charitable in the country, the investigation found, providing less financial aid as a percentage of their operating budgets on average than hospitals in almost every other state, including Illinois, Iowa, Nevada, and Texas.
The investigation drew on a detailed review of every hospital charity care program in the state, an analysis of five years of hospital financial data, and dozens of interviews with patients, hospital executives, and state officials.
Nationally, hospitals spend an average of about 2.4% of their operating budgets on charity care, according to federal hospital data compiled by Hossein Zare, a researcher at Johns Hopkins University. Minnesota hospitals spend about a third of that, on average.
Some spend considerably less. Of Minnesota’s 123 general hospitals, 62 devoted less than 0.5% of their operating budgets to charity care from 2020 through 2024, the Star Tribune-KFF Health News investigation found.
“The system is not working,” said Erin Hartung, director of legal services at Cancer Legal Care, a Minnesota nonprofit that helps patients with medical debt and other financial challenges. “And the burden is falling hardest on the people who are least able to bear it.”
CentraCare’s flagship St. Cloud Hospital spent less than 0.25%, according to the analysis. That works out to $25 in patient aid for every $10,000 spent on hospital operations.
Charity care will become even more vital in coming years as Minnesotans lose health coverage or can’t afford rising copays and deductibles. The state’s uninsured rate rose sharply last year, hitting its highest level since 2017, and it’s expected to increase further as budget cuts pushed by President Donald Trump force states to pare Medicaid and other safety net programs. Charity care is also critical to many people with health insurance who can’t afford their bills.
Hospital officials say it’s unfair to expect them to solve this affordability problem when many of their facilities are financially strained. “No amount of charity care from hospitals will ever fully meet the needs of uninsured or underinsured Minnesotans. The need is simply too great,” Minnesota Hospital Association spokesperson Tim Nelson said in a statement.
But state Attorney General Keith Ellison said hospitals have a duty to boost charitable help for all needy patients in exchange for the tax breaks they receive.
“There is a benefit you get from being a nonprofit hospital in the state of Minnesota,” he said. “But do the people get the benefit?”
Several small Minnesota hospitals give financial aid to fewer than two dozen patients a year. Mahnomen Health Center, which recently converted to a rural emergency center, didn’t provide any charity care in eight years, despite serving one of Minnesota’s most impoverished regions. Other hospitals serving large low-income populations were among those providing the least charity care, the analysis found.
Several factors help explain why Minnesota hospitals provide so little financial aid. For one, job-based insurance and an expanded Medicaid program offer broad coverage. Hospitals in states with less government assistance and more uninsured people typically spend more on charity care.
But Minnesota patients also face significant barriers accessing financial aid at many hospitals, including inconsistent eligibility standards and extensive applications, the Star Tribune-KFF Health News investigation found.
To qualify at many hospitals, patients must submit detailed personal information, including bank statements, retirement accounts, mortgage documents, and estimates of other assets such as cars, homes, or livestock.
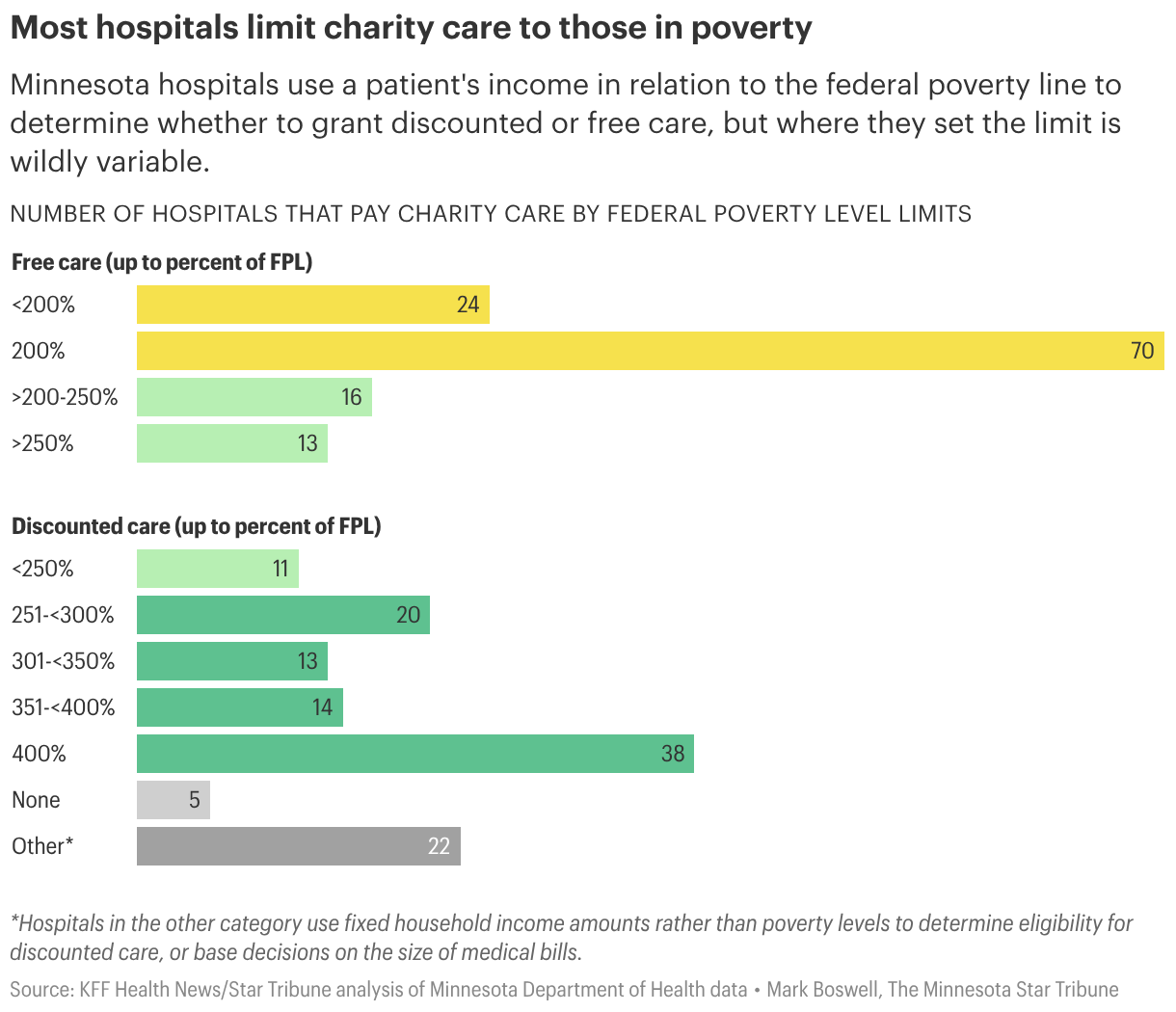
And because Minnesota has not standardized the criteria for charity care, patients might receive aid at one hospital but not another. The investigation found that some hospitals give free care to patients with an annual household income of $47,000, while others cap it at about $15,000.
Had Roberts driven 30 miles east to Princeton or 35 miles north to Little Falls, she would have found medical providers with more generous financial aid policies than CentraCare. But she didn’t know to look.
Roberts, now 49, has remarried and lives in a split-level home in St. Cloud decorated with inspirational plaques such as “Faith, Family, Friends.” CentraCare recently dropped the lawsuit against her, but only after she took out a loan against her retirement plan to pay off the medical debt. “It just feels very unfair,” she said.

‘We Have To Defend Being Paid’
CentraCare spokesperson Karna Fronden said medical privacy laws prevented her from discussing Roberts’ case. She also declined interview requests about the health system’s charity care spending.
In a statement, Fronden said CentraCare provides assistance in addition to charity care, such as helping enroll patients in insurance. “This helps provide broader, longer-term protection for patients,” she said.
Other hospital leaders said they serve their communities in ways besides forgiving medical bills, including training doctors and nurses and preserving money-losing services such as obstetrics and mental health care.
“Rural hospitals like ours are often portrayed as though we are sitting on piles of cash and simply choosing not to spend it on charity care. That is far from the reality,” said Robert Pastor, chief executive of Rainy Lake Medical Center in International Falls.
“We are the second- or third-largest employer in town, running on razor-thin margins while navigating escalating labor and supply costs and routine underpayment by public programs,” Pastor said. “Meanwhile, many health insurers post billions in profits.”
Hospitals typically are paid less for care provided to Medicare and Medicaid patients. More than 80% of Rainy Lake’s patients are on one of those government programs.
Minnesota hospitals collectively write off about $200 million of what’s deemed bad debt every year after trying unsuccessfully to collect unpaid bills from patients through calls, letters, and even lawsuits. By comparison, they devote about $163 million annually to charity care, state figures show. In 2024, hospitals collectively posted $2.4 billion in net income.
“I feel like I’m put in the position, being the hospital, where we have to defend being paid,” said Patti Banks, the head of Ely-Bloomenson Community Hospital and a senior Minnesota Hospital Association board member.
Some hospitals face intense financial pressures. Thirty-one have lost money on operations in four of the past eight years. HCMC in Minneapolis — the state’s largest safety net hospital, which provides the most charity care — is losing so much money that, without additional taxpayer support, it could close.
But larger health systems such as Mayo Clinic, Essentia Health, and Sanford Health have remained financially sound. And the operating margins at most CentraCare hospitals exceeded 10% in 2024, state data shows.
Medical Debt’s High Toll

Nationwide, health care debt — much of it from hospitals — burdens an estimated 100 million people, increasing their stress and even leading to premature deaths, studies show.
Abby Kelley-Hands, a special education coordinator in St. Paul, has a rare immune condition that causes frequent, severe allergic reactions. Her illness can be controlled only with a costly drug, which a Mayo Clinic doctor prescribed.
When Kelley-Hands briefly lost health coverage in 2021 in an insurance mix-up, she was hit with more than $20,000 in bills. And although she and her husband earned less than $100,000 a year, Kelley-Hands said Mayo denied her financial assistance because she earned too much.
“I was in tears,” Kelley-Hands said. “It was so scary and so hard. And it causes all of this additional stress, which then makes you sicker and less able to even figure things out.”
Kelley-Hands and her husband sold a car and agreed to a payment plan before Mayo would resume her treatment, she said. Her husband now bikes 5 miles to work. They have no dishwasher. And she and her husband took a honeymoon only last fall, seven years after their wedding. “We live very simply,” she said.
Mayo spokesperson Kristyn Jacobson declined to discuss Kelley-Hands’ case.
In 2024, state lawmakers banned hospitals from denying care to patients with outstanding debt. And in 2025, Attorney General Ellison reached an agreement with Mayo to overhaul its charity care program after an investigation found the multibillion-dollar institution was systematically discouraging patients from applying.
After the state began investigating Mayo, the system’s charity care spending nearly doubled, topping 1.5% of operating expenses in 2024.
‘Optimized To Get Payment’
Complying with a 2023 state law, Minnesota hospitals now post their financial aid policies online, although several, including CCM Health in Montevideo and Northfield Hospital, did so only after being contacted by the Star Tribune or KFF Health News.
But many hospitals make financial aid more difficult to find than information about paying bills, said Jared Walker, founder of Dollar For, a nonprofit that helps patients nationally apply for charity care.
“Hospitals have optimized to get payment,” he said. “If you want to get on a payment plan, if you want to get on a credit card, it’s so easy.”
Glacial Ridge Health System in Glenwood posts a “Bill Pay” tab at the top of its homepage. But it takes several clicks to find the hospital’s financial assistance plan. The information couldn’t be found on the site searching for “charity care” or “financial assistance.” The public hospital 130 miles northwest of Minneapolis devoted less than 0.7% of its operating budget to charity care from 2019 to 2024.
Patients in interviews frequently said they weren’t told about charity care.
Joe Robling, 29, was treated at St. Francis Regional Medical Center in Shakopee for a broken pelvis and fractured spine after a 2024 motorcycle accident. His mother, Janet, who helped him navigate the bills, said the hospital never informed him about financial aid.
“They didn’t offer any of that,” she said.
Robling, a construction worker in Henderson, was between jobs and uninsured. “He had zippo,” Janet Robling said. “What he had in reserves were all depleted.”
The Allina Health-affiliated hospital billed him more than $19,000, the Roblings said.
An internet ad connected the family to Dollar For, which helped Robling qualify for charity care five months after his accident.
Allina spokesperson Jennifer Steingas declined to comment on the case, citing medical privacy restrictions, but said the health system has since reached out to the family.
In another case, M Health Fairview’s University of Minnesota Medical Center didn’t offer financial aid to an unemployed and uninsured man from Idaho while he was hospitalized for two months for psychiatric care and amassed $150,000 in bills.
Attorney Margaret Henehan, who represented the man, said the hospital instead offered him a two-year payment plan at $6,500 a month. “He had no income, which he told Fairview,” Henehan said.
The man, who is not identified because of his mental health condition, eventually received charity care after his sister, a doctor, reached out to Henehan for help.
Aimee Jordan, a Fairview spokesperson, said she couldn’t comment on the case because of patient privacy laws, but she said patients who are offered payment plans can always apply for charity care, even after a hospitalization.

A Maze of Standards
State law prohibits hospitals from making “unreasonable” demands of patients when they apply for charity care. But the law sets few specific standards.
The result is a dizzying array of policies, including 11 income thresholds used by Minnesota hospitals to determine whether patients qualify for free care, the Minnesota Star-Tribune-KFF Health News review found.
HCMC parent company Hennepin Healthcare in Minneapolis and Olmsted Medical Center in Rochester offer the highest threshold for free care, at 300% of the federal poverty level — almost $48,000 a year for an individual.
Sometimes standards vary even between neighboring hospitals. Madelia Health in south-central Minnesota limits financial assistance to patients who make less than twice the federal poverty level. About 13 miles away at Mayo’s hospital in St. James, patients earning twice as much can qualify for aid.
To determine eligibility, some Minnesota hospitals consider only income, but most demand information about patients’ bank accounts as well. More than two-thirds require even more information, including the value of retirement accounts, life insurance policies, property, and vehicles. Madelia’s policy states patients “may be required to sell recreational vehicles.”
Stringent requirements ensure that limited resources go to patients who need them, said Travis Olsen, chief executive of Hendricks Community Hospital, near the South Dakota border. “We don’t feel it’s fair for someone with lower annual income but yet owns numerous acres of land, debt-free, to be able to qualify for charity care.”
In addition to copies of tax returns, W-2 forms, pay stubs, and bank statements, Hendricks asks aid applicants 53 questions about their finances. These include questions about the make, model, and value of vehicles; the current market value of farm equipment, livestock, and land; and the purchase price and square footage of homes.
Other hospital applications ask patients to detail their monthly spending on food, utilities, and other medical bills.
Olsen said community pressure is more of a deterrent to applying for aid than the application: “People are too proud to pick up an application. We all know each other.”
But Walker at Dollar For said the biggest barrier is complexity. “The drop-off rates are much higher the more questions you ask and the more documentation you have to provide,” he said.
Arleen Mullenax had a cancerous tumor removed from her neck at Mayo in Rochester. Assembling her aid application and following up with the hospital billing department amid her “cancer fog” was almost more than she could take, she said.
“I knew as a former office manager I had to stay on top of it,” she said. “But it was the most daunting thing I had to do as a patient.”

Fixing the System
Ellison and several state lawmakers say Minnesota’s hospitals should make it simpler for patients to access charity care.
They’ve called for, among other things, common eligibility standards and a standard application across hospitals. New York and Maryland already have both.
“Eliminating as many barriers as possible for people is really important,” said state Sen. Liz Boldon, who also said she hopes lawmakers can enact these standards next session.
The Minnesota Hospital Association has opposed standardizing financial assistance, saying hospital boards are in the best position to assess the need for charity care in their communities. “Adding mandates for providers across the state will not close that gap, and will only increase bureaucratic and procedural barriers to patient care,” spokesperson Nelson said.
Ellison also has pushed to require hospitals to use a process that automatically screens and qualifies low-income patients for financial aid without requiring an application.

Some hospital systems, including South Dakota-based Sanford Health, already use software that checks patients’ eligibility based on information such as their credit history, said Nick Olson, the system’s chief financial officer. At Sanford Health’s 10 hospitals in Minnesota, about a quarter of the patients who receive financial aid get it this way, he said.
Nearly all Sanford hospitals devote more than 1% of their operating expenditures to charity care — higher than most hospitals in the state.
Screening software can be costly. Several executives at small Minnesota hospitals said they can’t afford it. But there are other options. In California, Los Angeles County is developing a public system to allow hospitals to quickly assess patients’ eligibility so they don’t have to buy a system themselves.
Other states — including Texas and Nevada — have laws requiring hospitals to provide minimum amounts of charity care.
Back in St. Cloud, Roberts said that when she drives past CentraCare’s $200 million expansion at its Plaza campus in St. Cloud, she wonders why Minnesota hospitals don’t live up to higher standards themselves.
“They have all the money,” she said. “But they can’t grant a good person some grace?”