The Host
Julie Rovner
KFF Health News
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
At the Trump administration’s request, a federal judge in Louisiana this week agreed to delay a ruling affecting the continued availability of the abortion drug mifepristone. That angered anti-abortion groups that want the drug, if not banned, at least more strictly controlled. But the administration clearly wants to avoid big abortion fights in the run-up to November’s midterm elections.
Meanwhile, the administration’s proposed budget for fiscal year 2027 calls for more than $15 billion in cuts to programs at the Department of Health and Human Services. It’s a significant number, but less drastic than cuts it proposed for fiscal 2026.
This week’s panelists are Julie Rovner of KFF Health News, Lauren Weber of The Washington Post, Alice Miranda Ollstein of Politico, and Maya Goldman of Axios.
Panelists
Maya Goldman
Axios
Alice Miranda Ollstein
Politico
Lauren Weber
The Washington Post
Among the takeaways from this week’s episode:
- The Trump administration says it is conducting a thorough scientific review of the abortion pill mifepristone at the Food and Drug Administration. Yet advocates on both sides of the abortion debate think the administration is just trying to buy time to avoid a controversial decision about medication abortion before November’s midterm elections.
- It’s budget time on Capitol Hill. With the unveiling of the president’s spending plan for fiscal 2027, Cabinet secretaries will make their annual tour of congressional committee hearings. HHS Secretary Robert F. Kennedy Jr., whose Hill appearances have been few during his tenure, is scheduled to testify before six separate House and Senate committees before the end of the month.
- Back at HHS, Kennedy appears to be trying to reconstitute the Advisory Committee on Immunization Practices in a way that will enable him to restock it with vaccine skeptics without running afoul of a March court ruling that he violated federal procedures with his replacements last year.
- Continuing his efforts to promote his Make America Healthy Again agenda, Kennedy announced this week that he will launch his own biweekly podcast. He also announced efforts to combat microplastics in the water supply and to get hospitals to stop serving ultraprocessed food to patients.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week that they think you should read, too:
Julie Rovner: The Atlantic’s “HHS Officials’ Year in Purgatory Is Ending,” by Katherine J. Wu.
Maya Goldman: KFF Health News’ “Trump’s Personnel Agency Is Asking for Federal Workers’ Medical Records,” by Amanda Seitz and Maia Rosenfeld.
Lauren Weber: CNN’s “These Common Drug Tests Lead to Tens of Thousands of Wrongful Arrests a Year, Experts Say. One State Is Fighting Back,” by Holly Yan.
Alice Miranda Ollstein: Politico’s “A Slowdown in US Visa Processing Is Wreaking Havoc on Foreign Doctors’ Lives,” by Simon J. Levien.
Also mentioned in this week’s podcast:
Click to open the transcript
Transcript: Abortion Pills, the Budget, and RFK Jr.
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello, from KFF Health News and WAMU Public Radio in Washington, D.C. Welcome to What the Health? I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters covering Washington. We’re taping this week on Thursday, April 9, at 9:30 a.m. As always, news happens fast, and things might have changed by the time you hear this. So here we go.
Today, we are joined via video conference by Lauren Weber of The Washington Post.
Lauren Weber: Hello, hello.
Rovner: Alice Miranda Ollstein of Politico.
Alice Miranda Ollstein: Hi, everybody.
Rovner: And my fellow Michigan Wolverine this national championship week, Maya Goldman of Axios. Go, Blue!
Maya Goldman: Go, Blue.
Rovner: No interview this week, but plenty of news. So let’s get right to it. We’re going to start with reproductive health. On Tuesday, a federal judge in Louisiana ruled for the Trump administration and against anti-abortion forces in a lawsuit over the availability of the abortion pill mifepristone. Wait, what? Please explain, Alice, how the administration and anti-abortion groups ended up on opposite sides of an abortion pill lawsuit.
Ollstein: Yeah. So this has been building for a while, and it is not the only lawsuit of its kind out there. There are several. A bunch of different state attorneys general, who are very conservative and anti-abortion, have been suing the FDA in an attempt to either completely get rid of the availability of the abortion pill mifepristone or reimpose previous restrictions on it. So right now, at least according to federal rules, not according to every state’s rules, you can get it via telehealth. You can get it delivered by mail. You can pick it up at a retail pharmacy. You don’t have to get it in person handed to you from a doctor like you used to. So these lawsuits are attempting to bring back those restrictions or get the kind of national ban that a lot of groups want. And so you have other ones pending: Florida, Texas, Missouri, you have a bunch of ones. So this is the Louisiana version. And the Trump administration, it’s important to note, they are not defending the FDA or the abortion pill on the merits. They are saying, we don’t want this lawsuit and this court to force us to do something. We want to go through our own careful process and do our own internal review of the safety of mifepristone, and then we may decide to impose restrictions. But they’re asking courts to give them the time and space to complete that process and saying, you know, This is our power we should have in the executive branch. And so, in this case, the judge, in ruling for the Trump administration, basically just hit pause. This doesn’t get rid of the case. It just puts a stay on it for now, and that’s important. In some of these other cases, the Trump administration has asked the courts to throw out the case, but that was not the situation here. So this doesn’t mean that abortion pills are going to be available forever. This doesn’t mean nothing’s going to happen, and they’re going to be banned. This just means, you know, we’re kicking the can down the road.
Rovner: I was saying, just to be clear. I mean, we know that this FDA quote-unquote “study” — whether it is or isn’t going on — is part of, kind of, a delaying tactic by the administration, because they don’t want to really make abortion a big front-and-center issue in the midterms. So they’re trying to sort of run the clock out here. Is that not sort of the interpretation that’s going on right now?
Ollstein: That’s what people on both sides assume is going on. It’s really been fascinating how everyone is being kept in the dark about what’s happening inside the FDA — and if this review is even happening, if it’s real, if it’s in good faith, what is it based on? And so it’s become this sort of Rorschach test, where people on the left are saying, you know, They’re laying the groundwork to do a national ban. This is just political cover. They just want to wait until after the midterms, and then they’re going to go for it. And people on the right are saying, you know, The administration is cowardly, and they aren’t really doing anything, and they’re just trying to get us to shut up and be patient. We don’t know if either of those interpretations or neither of them are true.
Rovner: Lauren, you want to add something?
Weber: I just think it’s pretty clear this is also just on a [Health and Human Services Secretary Robert F.] Kennedy [Jr.] priority. I mean, let’s go back. The man … comes from one of the top Democratic political families originally. You know, there’s obviously been a lot of chatter around his anti-abortion beliefs. Now, obviously, he’s on a Republican ticket. I think some of that plays into this as well. And he already has his hand on the stove on so many other hot issues that, [if] I had to guess, I don’t think that they’re trying to rock the boat on this one. … I think, some background context too, to some of what’s going on.
Rovner: We’ll get to some of those hotter issues. But, meanwhile, the Journal of the American Medical Association [Internal Medicine] has a study out this week suggesting that medication abortion is so safe that it could be provided over the counter — that’s without any consultation with a medical professional, either in person or online. This doesn’t feel like it’s going to happen anytime soon, though, right? While we’re still debating the existence of medication abortion in general.
Ollstein: That’s right. I mean, there are a lot of people who can’t get this medication prescribed by a valid doctor right now, let alone over the counter. I will say it is common in a lot of parts of the world to get it over the counter, whereas in the United States, the most common way to have a medication abortion is with a two-pill combination, mifepristone and misoprostol. In a lot of parts of the world, people just use misoprostol alone, and it is effective and it is largely safe. It’s slightly less safe than using both pills together. And so I think there’s a lot of international data out there, and people point to that and advocate for this. And I will say there are activist groups in the United States who are setting up networks, underground networks, to get these pills to people with no doctor’s involvement. And so that is already going on. I think that a lot of people would prefer to get it from a doctor if they could. But because of bans and restrictions, they can’t. And so people are turning to these activist groups.
Rovner: I will point out, as a person who covered the entirety of the fight to have emergency contraception — which is not the abortion pill — made over the counter, it took like, 15 years. It shortened my life covering that story. Lauren, did you want to add something?
Weber: Yeah, I just wanted to say I find it really interesting. Obviously, reproductive issues end up taking 15 years, as you pointed out, to make it over the counter. But there are a lot of things that are considered potentially more dangerous that you can order up in a pretty basic telehealth visit or even just buy in not-so-sketchy ways that the administration is also even looking to deregulate. So I think the differences of access of this compared to other less studied, potentially more unsafe medication is quite striking.
Goldman: Part of [President Donald] Trump’s “Great Healthcare Plan” is making more medications available over the counter. So this is certainly something that they have said they want to do, in general. This is a political nightmare, though, to do that for abortion.
Ollstein: Yeah, and people have been pointing to this and a lot of other policies for a while to argue about something they call abortion exceptionalism, in which people apply a different standard to anything related to abortion, a different safety standard, a different standard of scrutiny than they do to medications for lots of other purposes. And you’ve seen that, and that comes up in lawsuits and political arguments about this. And I think, you know, people can point to this as another example.
Rovner: So last week, we talked about the federal family planning program Title X, which finally got funded after months of delays. But Alice, you warned us that the administration was planning to make some big changes to the program, and now those have finally been announced. Tell us what the plan is for a program that’s provided birth control and other types of primary and preventive care since the early 1970s.
Ollstein: Well, the changes have sort of been announced. They’ve more been teased. What we are still waiting for is an actual rule, like we saw in the first Trump administration, that would impose conditions on the program. And so what we saw recently, it was part of a wonky document called a “Notice of Funding Opportunity,” or NOFO, for those in the D.C. lingo. And basically it was signaling that when groups reapply — they just got this year’s money, but when they reapply for next year’s money — it sets up sort of new priorities and a new focus for the entire program. And what was really striking to me is, you know, this is a family planning program. It was created in the 1970s and it is primarily about delivering contraception to people who can’t afford it around the country, providing it to millions of people who depend on this program, and the word “contraception” did not appear in the entire 70-page document other than an assertion that it is overprescribed and has bad side effects. And instead, they signaled that they want to shift the program to focus on, quote, “family formation.” So this is really striking to me. I think we saw some signs that something like this was coming. You know, about a year ago, there was some Title X money approved to focus on helping people struggling with infertility. But that was sort of just a subset of the program, and now it looks like they want to make that, you know, an overriding focus of the program. So I think when the actual rule to this effect drops, and we don’t know when that will be — will they wait till after the midterms to, you know, avoid blowback? Who knows? I think there will certainly be lawsuits then. But I think right now, this is just sort of a sign of where they want to go in the future. And it’s important to note that it came very quickly on the heels of a big backlash from the anti-abortion movement over the approval of this year’s funding going out to all of the clinics that got it before, including Planned Parenthood clinics. The anti-abortion groups were agitating for Planned Parenthood to be cut off at once, you know, not in the future, right now.
Rovner: Just to remind people that the ban on Planned Parenthood funding from last year was for Medicaid, not for the Title X program.
Ollstein: Right.
Rovner: And that’s why Planned Parenthood got money.
Ollstein: Yes, and Planned Parenthood is not allowed to use any Medicaid or Title X money for abortions, but the anti-abortion groups say it functions like a backdoor subsidy, and so they wanted it to be cut off. So they were very pissed that this money went out to Planned Parenthood. And so very quickly after, the administration put out this document, saying, Look, we are taking things in another direction, and it is not the direction of Planned Parenthood.
Rovner: Lauren, you want to add something?
Weber: Oh, I just wanted to say Alice has really been owning the beat on all the Title X coverage, so …
Rovner: Absolutely.
Weber: … glad we are able to have her explain it to us. But just wanted to throw out a kudos for breaking all the news on that front.
Goldman: Yeah, great coverage.
Rovner: Yes. Very happy to have you for this. Turning to the budget, which is normally the major activity for Congress in the spring, we finally got President Trump’s spending blueprint last week. It does propose cuts to discretionary spending at the Department of Health and Human Services to the tune of about $15 billion, but those cuts are far less deep than those proposed last year. And, as we have noted, Congress didn’t actually cut the HHS budget last year by much at all. And many programs, like the National Institutes of Health, actually got small increases. Is this budget a reflection of the fact that the administration is recognizing that cuts to Health and Human Services programs aren’t actually popular with the public or with Congress, for that matter, going into a midterm election?
Weber: I think it’s that last little piece you mentioned there, Julie. I think it’s the “going into the midterm election.” I think you hit the nail on the head there. Cuts are also not good economically for many Republicans. You know, we saw Katie Britt be one of the — the Alabama Republican senator — be one of the most outspoken senators in general about some of the cuts that were floated for the budget for HHS last year. So I think what you’re hinting at, and what we’re getting at, is that it’s not politically popular, it can be economically problematic, on top of the scientific advances that are not found. So I suspect you are right on that.
Ollstein: The administration knows that this is “hopes and dreams” and will not become reality. It did not become reality last year. It almost never becomes reality. And I think you can see the sort of acknowledgement that this is about sending a message more than actually making policy in things like Title X, because at the same time they put out this guidance from HHS about the future of Title X, moving away from contraception, in the president’s budget he proposed completely getting rid of Title X, completely defunding it, which he has in the past as well. And so why would they put out guidance for a program that doesn’t exist?
Goldman: I think, also, this is the second budget that they’re putting out in this administration, right? So now they are just a little more used to what’s going on, and they have more of their feet under them.
Weber: As a preview for listeners, too, I’m sure we will have Kennedy asked about this budget when he appears in a series of so many hearings next week and the week after. And there were a lot of fireworks last year with him and various members of Congress about the budget. So I am sure that we will hear a lot more on this front in the weeks to come.
Rovner: Yeah, I would say that’s one thing that the budget process does, is when the president finally puts out a budget, the Cabinet secretaries travel to all of the various committees on Capitol Hill to, quote, “defend the president’s budget,” which is sometimes or, I guess in the case of Kennedy, one of the few chances that they get to actually have him in person to ask him questions. But in the meantime, you know, we have the budget, then we have the president himself, who at an Easter lunch last week — that was supposed to be private, but ended up being live-streamed — said, and I quote, “It’s not possible for us to take care of day care, Medicare, Medicaid, all these individual things.” The president went on to say that states should take over all that social spending, and the only thing the federal government should fund is, quote, “military protection.” Did I just hear a thousand Democratic campaign ads bloom?
Goldman: I think this is a prime example of when you should take Trump seriously, but not literally. I don’t think that there’s any world, at least in the foreseeable future, where the federal government isn’t funding Medicare. But, you know, you certainly have to watch at the margins. It’s like, it’s not a secret that this is something that they’re interested in cutting back spending on. It’s super politically difficult to do that, and they know that, and that’s part of why, which I’m sure we’ll talk about in a little bit, they bumped up the payment rate for 2027 to Medicare Advantage plans.
Rovner: Which we will get to.
Goldman: Yeah, so I mean, it’s certainly an eye-opening statement, and you should remember it. But I don’t think that we’re in immediate jeopardy here.
Rovner: This is the president who ran in 2024, you know, saying that he was going to protect Medicare and Medicaid. I mean, it’s been, you know, against some of the recommendations of his own administration. I was just sort of shocked to see these words come out of his mouth. Lauren, you wanted to say something?
Weber: I mean, it’s not that surprising, though. I mean, look at what the One Big Beautiful Bill [Act] did to Medicaid. He’s already pushed through massive Medicaid cuts, which are essentially being offloaded to the states. So, I mean, I think this ideology has already borne out and will continue to bear out, and obviously it’s happening amid the backdrop of a war. So that plays into, obviously, the commentary as well.
Rovner: Well, meanwhile, Republicans are still talking about doing another budget reconciliation bill, the 2.0 version of last year’s Big Beautiful Bill, except this time it’s essentially just to fund the military and ICE [Immigration and Customs Enforcement] and border control, because Democrats won’t vote for those things, at least they won’t vote for additional military spending. What are the prospects for that to actually happen? And would Republicans really be able to do it if those programs are paid for with more cuts to Medicare and/or Medicaid, as some have suggested?
Goldman: You know, my co-worker Peter Sullivan wrote about this last week, and there was a lot of blowback from politicos, from advocates, from, you know, kind of across the spectrum of groups there. I think that it would be extremely politically unpopular, especially going into the midterms, to use health care as an offset. But I would say that Republicans are pretty good at rhetoric, right? That’s one of the things that they’re known for right now, and there’s always a way to spin it.
Rovner: Alice and I spoke to a group earlier this week, and I went out on a limb and predicted that I didn’t think Republicans could get the votes for another big budget reconciliation this year. I mean, look at how close it was last year. The idea of cutting any deeper seems to me unlikely, just given the margins that they have.
Goldman: And I think that is something that you do in between election years. That’s not something you do in an election year.
Rovner: That’s true, yes … you do tend to see these bigger bills in the odd-numbered years rather than the even-numbered years, but …
Ollstein: And I think it’s important to remember that the reason Republicans are in this bind and that they feel like they have to keep reconciliation nearly focused on funding immigration enforcement is because Democrats refuse to fund immigration enforcement. And so they feel pressured to put all their effort and political capital towards that, and don’t want to mess that up by adding a bunch of other health care things that could cause fights and lose them votes.
Goldman: The money has got to come from somewhere.
Rovner: And health care is where all the money is. Speaking of Medicare and Medicaid, where most of the money is, there is news on those fronts, too. Maya, as you hinted on Medicare, the administration is out with its payment rule for private Medicare Advantage plans for next year. And remember, we talked about how HHS was going to really go after overbilling in Medicare Advantage and cut reimbursement dramatically? Well, you can forget all that. The final rule will provide plans with a 2.48% pay bump next year. That’s compared to the less than 1% increase in the proposed rule. That’s a difference of about $13 billion. The final rule also eliminated many of the safeguards that were intended to prevent overbilling. What happened to the crackdown on Medicare Advantage? Are their lobbyists really that good?
Goldman: Their lobbyists are pretty good. This was a year where there were — I think CMS [the Centers for Medicare & Medicaid Services] said there were a record number of public comments on their proposed rate, flat rate increase, flat rate update. But I think it’s also not that surprising. Historically, the final rate announcement for Medicare Advantage is almost always a little higher than the proposed because they incorporate additional data from the end of the previous year that wasn’t available when first rate is proposed, the initial rate is proposed. But certainly they backed away from a big change to risk adjustment, or, like, the way to adjust payment based on how sick a plan’s enrollees are. You get more pay …
Rovner: Because that’s where the overbilling was happening, that we’d seen a lot of these wonderful stories that plans were basically, you know, inventing diagnoses for patients who didn’t necessarily have them or didn’t have a severe illness, and using that to get additional payments.
Goldman: Right. And they did move forward with a plan to prevent diagnoses that are not linked to information that’s in a patient’s medical chart from being used for risk adjustment. But a lot of plans had said, like, Yeah, this is, that’s the right thing to do, and it’s not going to be that impactful for us. You know, overall, this is a win for health insurance. I think one thing to note is that Chris Klomp, the director of Medicare, said, We’re still really focused on trying to right-size this program. That’s still a priority for us as an administration, but we also want to safeguard it. And so I think insurers are not off the hook entirely. There’s still going to be a lot of scrutiny, but their lobbyists are pretty good. And you know, no one wants to be seen as the candidate that cuts Medicare.
Rovner: And we have seen this before, that when Congress cuts “overfunding” for Medicare Advantage, the plans, seeing that they can’t make its big profits, drop out or they cut back on those extra benefits. And the beneficiaries complain because they’re losing their plans, or they’re losing their extra benefits, and they don’t really want to do that in an election year either, because there are a lot of people, many millions of people, who vote who are on these plans. So, in some ways, the plans have the administration over a political barrel, in addition to how good their lobbyists are.
Well, apparently, one group that HHS is still cracking down on are legal immigrants with Medicare. Most of the publicity around the health cuts in last year’s budget bill focused on the cuts to Medicaid. But we at KFF Health News have a story this week about legal immigrants who’ve paid into the Medicare system with their payroll taxes for years and are now being cut off from their Medicare coverage. This is apparently the first time an entire category of beneficiaries are having their Medicare taken away. I’m surprised there hasn’t been more attention to this, or if it’s just too much all happening at once.
Ollstein: I mean, there’s a lot happening at once, and even just in the space of immigrants’ access to health care, there is so much happening at once. And so this is obviously having a huge impact on a lot of people, but so are 100 other things. And I think, you know, the zone has been flooded as promised. And really, state officials who are also dealing with a thousand other things, Medicaid cuts, you know, these federal changes, work requirements, are grappling with this as well.
Rovner: Lauren, you wanted to add something?
Weber: Yeah. I mean, I thought it was, there was a striking quote in the story from Michael Cannon, who basically said, The reason this isn’t resonating is because this won’t upset the Republican base. And I think that’s a striking quote to be considered.
Rovner: Michael Cannon, libertarian health policy expert, just kind of an observer to this one. But yeah, I think that’s true. I mean, or at least the perception is that these are not Republican voters, although, you know, as we’ve seen, you know, Congress has tried to take aim at people they think aren’t their voters, and it’s turned out that those are their voters. So we will see how this all plays out.
Well, at the same time that this is all going on, the folks over at the newsletter “Healthcare Dive” are reporting that the Centers for Medicare & Medicaid Services are trying to embark on all these new initiatives on fraud, and work requirements, and artificial intelligence with a diminished workforce. While CMS lost far fewer workers in the DOGE [Department of Government Efficiency] cuts last year than many other of the HHS agencies — it was in the hundreds rather than the thousands — CMS has long been understaffed, given the fact that it manages programs that provide health insurance to more than 160 million Americans through not just Medicare and Medicaid, but also the Children’s Health Insurance Program and the Affordable Care Act. I know last week, FDA Commissioner Marty Makary said he wants to hire more workers to replace the 3,000 who were RIF’ed or took early retirement there at the FDA. And CMS does have lots of job openings being advertised. But it’s hard to see how replacing trained and experienced workers with untrained, inexperienced ones are going to improve efficiency, right?
Goldman: Tangentially, I was talking to a health insurance executive yesterday who was saying that his team is so much bigger than CMS, and they cover a fraction of the market, and they’re often the ones coming to CMS and proposing ideas and working with CMS on it. I don’t, I think that is a dynamic that far predates this administration, but …
Rovner: Oh, absolutely.
Goldman: But it’s certainly interesting. And … CMS has very ambitious plans, and not that many people to carry them out. But, you know, I think one thing that I also want to note is that when I talk to trade associations and stakeholders about this CMS, they are generally like, pretty support- … like, they say that they think they’re being heard, and they think that CMS and the career staff are doing, you know, the same kind of caliber of work that they’ve been doing, which I think is notable.
Rovner: And as we have mentioned many times, you know, Dr. [Mehmet] Oz, the head of CMS, is very serious about his job and doing a lot of really interesting things. It’s just, it’s hard, you know, in the federal government, if you don’t have the resources that you want to … if you don’t have the resources to match your ambitions. Let’s put it that way.
Well, meanwhile, on the Medicaid front, we’re already seeing states cutting back, and some of the results of those cutbacks. Stateline has a piece on how psychiatric units are at risk of being shut down due to the Medicaid cuts, since they often serve a disproportionate number of low-income people and also tend to lose money. And The New York Times has a heartbreaking story of an Idaho Medicaid cutback of a program that had provided home visits to people living in the community with severe mental illness, until those people who lost the services began to die or to end up back in more expensive institutional care. Now the state has resumed funding the program, but obviously will end up having to cut someplace else instead. I know when Republicans in Congress passed the cuts last year, they said that people on Medicaid who were not the able-bodied working-age populations wouldn’t see their services cut. But that’s not how this is playing out, right?
Weber: I just think the story by Ellen Barry, who you should always read on mental health issues in The New York Times, “Idaho Cut Services for People With Schizophrenia, Then the Deaths Began,” is such an illustrative example of unintended consequences from these cuts. And the reason that they’re being reversed — by Republican legislators, no less — in Idaho, is because it’s more expensive to have cut the money from it than it is efficient. I mean, what they found was, is that after they cut the money to the schizophrenia program, they saw this massive uptick in law enforcement cases and hospitalizations, uninsured hospitalizations, that this avoided. And I think it’s a real canary in the coal mine situation, because we’re only starting to see these states cut these things off. And this was a pretty immediate multiple-death consequence. And I think we’re going to see a lot of stories like this, of a variety of programs that we all don’t even have any idea that exist in the safety net across the country that are being chipped away at.
Rovner: Well, turning to other news from the Department of Health and Human Services, we’re getting some more competition here at What the Health? Health secretary Kennedy has announced he’ll be unveiling his own podcast, called The Secretary Kennedy Podcast, next week. He promises to, according to the trailer posted online on Wednesday, quote, “name the names of the forces that obstruct the paths to public health.” OK then, we look forward to listening.
Meanwhile, in actual secretarial work, the secretary this week also unveiled changes to the charter of the Advisory Committee on [Immunization] Practices after a federal judge last month invalidated both the replacement members that he’d appointed last year and the changes made to the federally recommended vaccine schedule. So what’s going to happen here now? Will this get around the judge’s ruling by watering down the expertise that members of this advisory committee are supposed to have in vaccines? And why hasn’t the administration appealed the judge’s ruling yet?
Goldman: You know, I don’t have actual answers to this, but I do wonder and speculate that this is going to end up being some kind of legal whack-a-mole situation where the secretary and HHS says, OK, you don’t like it that way? We’ll do it this way, and then they’ll do it another way, and advocates will sue, and we’ll see how this plays out going forward in the courts. I think this is not the end of the story. Even though the judge’s decision was a big win for vaccine advocates, it’s just we’re in the midpoint, if that.
Rovner: And Lauren, speaking of vaccines, your colleague Lena H. Sun has quite the scoop on HHS and vaccine policy.
Weber: Yeah, Lena Sun is always delivering. She found out that the acting director of the CDC [Centers for Disease Control and Prevention] at the time delayed publication of a report showing that the covid-19 vaccine[s] cut the likelihood of emergency department visits and hospitalizations for healthy adults last winter by about half. So even though Kennedy is not talking more about vaccines, it appears that, based on this reporting, that some of his underlings are not necessarily touting the benefits of vaccine, so to speak. And I’m very curious, going back to Kennedy’s podcast, I found the rollout of that so interesting because the teaser was very leaning into the Kennedy that got elected, you know, someone who speaks about, you know, dark truths that are hidden from the public, and so on. And then the press team had these statements of, like, Kennedy will investigate the affordability of health costs and food and nutrition. And I think this dichotomy of who Kennedy is and who the White House and the press secretary and HHS want Kennedy to be before the midterms really could come to a head in this podcast. So I think we will all be listening to hear how that goes.
Rovner: Yeah, we keep hearing about how the secretary is being, you know, sort of put on a leash, if you will. And, you know, told to downplay some of his anti-vaccine views and things like this. And that seems quite at odds with him having his own podcast. Alice, do you want to …?
Weber: I guess, it depends on who’s editing the podcast and who they have on. I’m just very … you could even tell from the trailer to how his press secretary presented it, there was an interesting differential in framing, and I am curious how that plays out as we see guests on it.
Ollstein: I mean, it’s also worth noting that this is an administration of podcasters. I mean, you have Kash Patel, you have so many of these folks who have a history of podcasting, clearly have a passion for it, just can’t let it go while working a full-time, high-pressure government job.
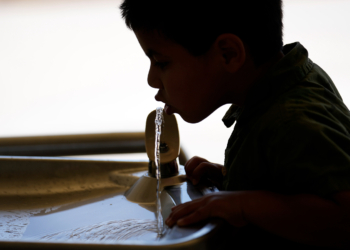
Rovner: We shall see. Meanwhile, HHS, together with the Environmental Protection Agency, is waging war on microplastics, those nearly too impossible to detect bits of plastic that are getting into our lungs and stomachs and body tissues through air and water and food. The plan here seems to be to find ways to detect exactly how much microplastics we are all getting in our water and what the health impacts might be, since we don’t have enough information to regulate them yet. I would think this would be one of those things that pleases both MAHA [Make America Healthy Again] and the science community, right? Or is it just, as one MAHA supporter called it, theater?
Goldman: I think this is a great example of the, you know, part of the reason why MAHA is so interesting to such a wide swath of people. Like, there’s a lot of legitimate concern, not that other concerns aren’t necessarily legitimate, but there’s a lot of concern over, from the scientific community, over microplastics. I’m honestly surprised that we’re this far into the administration with this announcement. I would have thought that this is something they would have done sooner, but they obviously had other priorities as well.
Rovner: Well. Finally, this week, speaking of other priorities, HHS Secretary Kennedy and CMS Administrator Dr. Oz are declaring war on junk food in hospitals. Again, this seems like a popular and fairly harmless crusade; hospitals shouldn’t be serving their patients ultraprocessed food. Except, almost as soon as the announcement came out, I saw tons of pushback online from doctors and nurses who worried about patients for whom sugary food or drinks are actually medically indicated, or who, because of medications they’re taking, or illnesses they have, can only eat, or will only eat, highly palatable, often processed food. Nothing in health care is as simple as it seems, right?
Weber: I think what’s also interesting is one of my favorite examples in the memo they put out was they hope that every hospital, as an example, could serve quinoa and salmon. And I just am curious to see how fast that gets implemented. And it’s a very valid — a lot of people complain about hospital food. It’s a very valid thing to push for better food. But I also question, as I understand it, this seems more like a carrot than a stick when it comes to the regulation they put out.
Rovner: As it were.
Weber: As it were. And so I’m curious to see how it gets implemented. That said, there are hospitals that have taken it upon themselves — the Northwell [Health] example in New York is a good example — to really improve their hospital food. And frankly, it’s a money maker. If your food’s better, people come to your hospital, especially in an urban area where there is hospital competition. So you know, like most MAHA topics, there’s a lot of interesting points in there, and then there’s a lot of what’s the reality and what’ actually going to happen. And so I’ very curious to see how this continues to play.
Rovner: I did a big story, like, 10 years ago on a hospital chain that had its own gardens, that literally grew its own healthy food. So this is not completely new but, again, interesting.
All right, that is this week’s news. Now it’s time for our extra-credit segment. That’s where we each recognize a story we read this week we think you should read, too. Don’t worry if you miss it. We will post the links in our show notes on your phone or other mobile device. Alice, why don’t you start us off this week?
Ollstein: I have a piece from my co-worker Simon [J.] Levien, and it is called “A Slowdown in US Visa Processing Is Wreaking Havoc on Foreign Doctors’ Lives.” This is about thousands of doctors around the country who are from other countries that are placed on, you know, a list by the Trump administration of places where they want to scrutinize and limit the number of immigrants coming from there. And so these are people who are already here, already practicing, have poured years into their training, have been living here, and, in some cases, are the only folks willing to work in certain areas that have a lot of medical shortages, and they just can’t practice because their paperwork isn’t getting processed in time. And so they’re sort of in this scary limbo, and that’s putting these hospitals and clinics that they work in in a really tough bind. And so they’re hammering the Trump administration to give them answers about what their fate is. You know, they’re not trying to deport them yet, but they’re not allowing them to continue working either.
Rovner: For an administration that’s been pushing really hard to improve rural health care, this does not seem to be a way to improve rural health care. Maya.
Goldman: My extra credit this week is called “Trump’s Personnel Agency Is Asking for Federal Workers’ Medical Records.” It’s a great KFF Health News scoop from Amanda Seitz and Maia Rosenfeld. It’s a really great example of the administration, you know, sort of moving in silence, doing these small regulatory announcements that could have big impact. Basically, the Office of Personnel Management is asking for personally identifiable medical information from health insurers, and its reasoning is to analyze costs and improve the health system, but they could get very detailed medical information from federal employees, including things like, did they get an abortion? Are they undergoing gender-affirming care? And, obviously, there is a strong concern that that could be used against them.
Rovner: Yeah … this was quite a scoop. Really, really interesting story. Lauren.
Weber: Mine was a pretty alarming story by Holly Yan at CNN: “These Common Drug Tests Lead to Tens of Thousands of Wrongful Arrests a Year, Experts Say. One State Is Fighting Back.” And basically there’s this type of drug test that the scientists have found is not that effective, and it’s led to things like bird poop being scraped off a man’s car appearing on a drug test as cocaine, a great-grandmother’s medication testing positive for cocaine, and a toddler’s ashes registering as meth or ecstasy, and horrible legal and other consequences of this kind of misdiagnosis in the field. And the reason these drug tests are often done is because they’re cheaper. There’s a more expensive, more accurate version, but these are cheaper. They’re done in the field. But the potential side effects and horrible, wrongly accused effects are quite large, and so Colorado has passed this law to try and move away from this. And it’s curious to see if other states will follow suit.
Rovner: Yeah, this was something I knew nothing about until I read this story. My extra credit this week is from The Atlantic by Katherine [J.] Wu, and it’s called “HHS Officials’ Year in Purgatory Is Ending.” And it’s about how some of the very top career officials from the NIH [National Institutes of Health], the CDC, and other agencies have, after having been put on leave more than a year ago, finally been reassigned to far-flung outposts of the Indian Health Service in the western United States. They got news of their proposed reassignments with little description of their new roles and only a couple of weeks to decide whether to move across the country or face termination. Now, if these officials’ skills matched those needed by the Indian Health Service, this all might make some sense. But what the IHS most needs are active clinicians: doctors and nurses and social workers and lab technicians. And those who are now being reassigned are largely managers, including — and here I’m reading from the story, quote — “the directors of several NIH institutes, leaders of several CDC centers, a top-ranking official from the FDA tobacco-products center, a bioethicist, a human-resources manager, a communications director, and a technology-information officer.” The Native populations who are ostensibly being helped here aren’t very happy about this, either. Former Biden administration Interior Secretary Deb Haaland, a Native American who’s now running for governor in New Mexico, called the reassignment proposals, quote, “shameful” and “disrespectful.” Also, and this is my addition, not a very efficient use of human capital.
OK, that’s this week’s show. Thanks this week to our fill-in editor, Mary-Ellen Deily, and our producer-engineer, Francis Ying. A reminder: What the Health? is now available on WAMU platforms, the NPR app, and wherever you get your podcasts — as well as, of course, kffhealthnews.org. Also, as always, you can email us your comments or questions. We’re at whatthehealth@kff.org. Or you can find me on X @jrovner, or on Bluesky @julierovner. Where do you guys hang these days? Maya.
Goldman: I am on LinkedIn under my first and last name, Maya Goldman, and on X at @mayagoldman_.
Rovner: Alice.
Ollstein: I’m on Bluesky @alicemiranda and on X @AliceOllstein.
Rovner: Lauren.
Weber: Still @LaurenWeberHP on both X and Bluesky.
Rovner: We will be back in your feed next week. Until then, be healthy.
Credits
Francis Ying
Audio producer
Mary-Ellen Deily
Editor
Click here to find all our podcasts.
And subscribe to “What the Health? From KFF Health News” on Apple Podcasts, Spotify, the NPR app, YouTube, Pocket Casts, or wherever you listen to podcasts.